|
Interpret the meaning of 20/20 vision |
|
Normal visual acuity is 20/20. The top number indicates the distance the person is standing from the chart and the donominator gives the distance which a normal eye could have read that particular line. 20/20 means you can read at 20 feet what the normal eye can read at 20 feet. |
| |
|
Snellen eye chart |
|
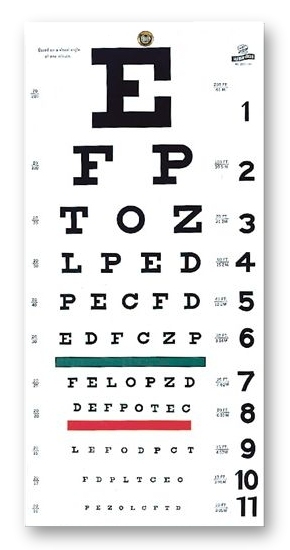
Most commonly used and accurate measure of visual acuity. It has lines of letters arranged in decreasing size. Normal vision is 20/20. |
| |
|
Near Vision Test |
|
Purpose: To screen people over 40 or people having difficulty reading near vision. Test near vision with a handheld vision screener with various sizes of print. Have the person hold the card about 14 inches away. Test each eye separately. Expected findings: A normal result is 14/14 in each eye, read without hesitancy, and without moving the card closer or farther away. |
| |
|
Corneal LIght Reflex |
|
Purpose: to assess the parallel alignment of eyes by shining a light toward the person's eyes.To perform: Direct the person to stare ahead as you hold the light about 12 inches away. The reflection of the light on the corneas should be in the exact same spot on each eye (symmetrical). |
| |
|
Pupillary Light Reflex |
|
This is the normal constriction of the pupils when bright light shines on the retina. Purpose: This tests the function of the cranial nerve, the optic nerve, and the oculomotor nerve because these nerves are required for the reflex to occur. To perform: Expose one eye to the bright light and observe for constriction of that pupil and the simultaneous constriction of the other pupil. Expected findings: When one eye is exposed to bright light, both pupils will constrict. |
| |
|
Cover Test |
|
Purpose: To detect small degrees of deviated alignment by interrupting the fusion reflex that normally keeps the two eyes parallel. To perform: Ask the person to stare straight ahead at your nose even though the gaze may be interrupted. With an opaque card, cover one eye. As it is covered, note the uncovered eye. Expected findings: A normal response is a steady fixed gaze. Now, uncover the eye and observe it for movement. It should be staring straight ahead. If it jumps to re-establish fixation, eye muscle weakness exists. Repeat with other eye. |
| |
|
Accommodation Test |
|
Purpose: To test for accommodation: the adaptation of the eye for near vision. To perform: Ask the person to focus on a distant object. This process dilates the pupils. Then have the person shift the gaze to a near object, such as your finger held about 8 cm from nose. Expected findings: A normal response includes 1. pupillary constriction 2. convergence of the axes of the eyes. |
| |
|
PERRLA |
|
The method for recording the normal response to all these maneuvers: P=PupilsE=EqualR=RoundR=React to L=LightA=Accommodations
|
| |
|
Collect subjective history information concerning eye and vision |
|
1. Vision difficulty (decreased acuity, blurring, blind spots)2. Pain3. Strabismus, diplopia4. Redness, swelling5. Watering, discharge6. Hx of ocular problems7. Glaucoma8. Use of glasses/contacts9. Self-care behaviors |
| |
|
Inspect external eye structure |
|
GeneralEyebrowsEyelids and lashesEyeball alignmentConjunctiva and scleraLacrimal apparatus
|
| |
|
Inspect anterior eyeball structures |
|
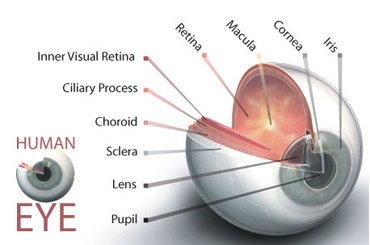
Cornea and lensIris and pupil (size, shape, equality, pupillary light reflex, accommodation)
|
| |
|
Inspect ocular fundus |
|
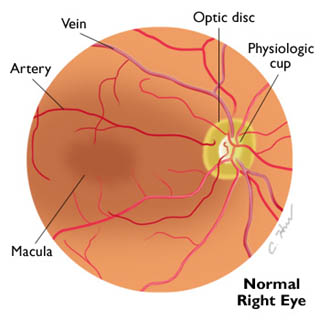
Optic disc (color, shape, margins, cup-disc ratio)Retinal vessels (number, color, artery-vein ratio, caliber, arteriovenous crossings, tortuosity, pulsations)General background (color, integrity)Macula |
| |
|
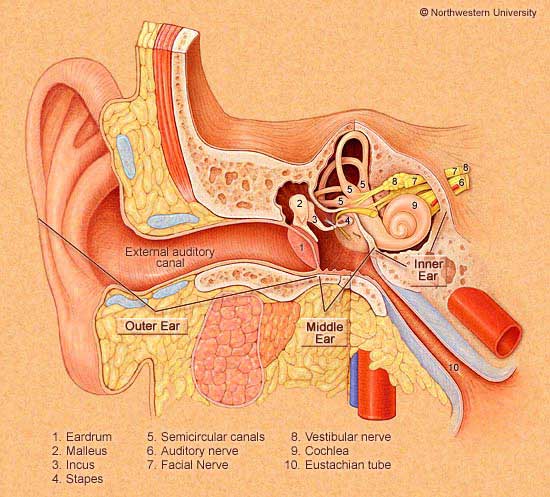
External auditory canal |
|
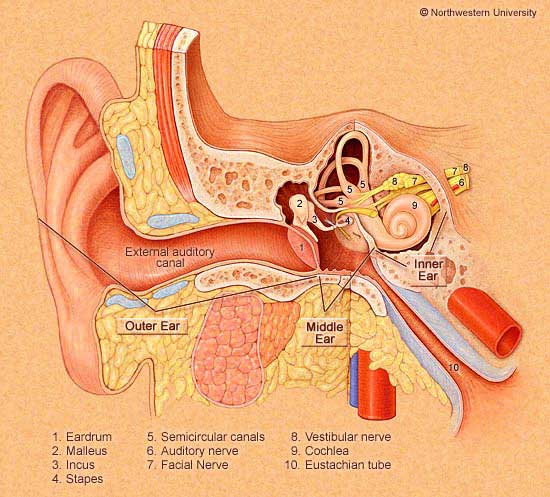
Opening through which sound waves are funneled into the ear. The canal is a cul-de-sac 2.5-3cm long and terminates at the eardrum. It is lined with glands that secrete cerumen (ear wax) |
| |
|
Tympanic membrane |
|
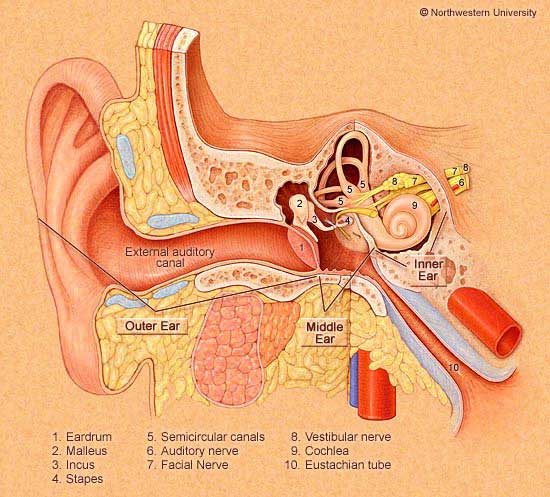
aka eardrumSeparates the external and middle ear and is titled obliquely to the ear canal, facing downward and somewhat forward. The drum is oval and slightly concave |
| |
|
Malleus |
|
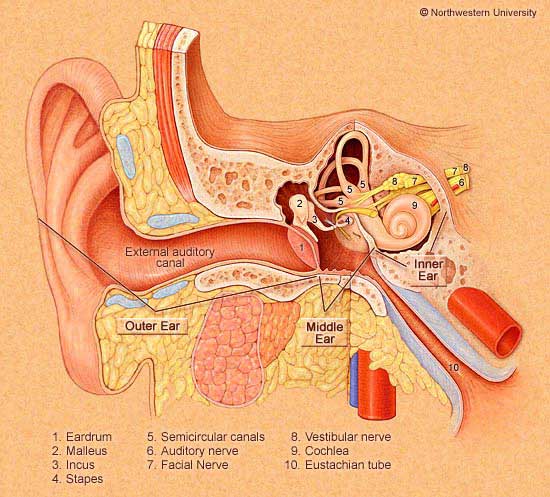
A middle ear ossicle that pulls the eardrum in at its center. It has 3 parts: the umbo, the manubrium (the handle), and the short process. |
| |
|
Annulus |
|
outer fibrous rim of the drum |
| |
|
Parts of the inner ear |
|
1. bony labyrinth: holds the sensory organs for equilibrium and hearing2. vestibule and semicircular canals: compose the vestibular apparatus and found within the bony lab3. cochlea: latin for snail shell. contains the central hearing apparatus |
| |
|
Infant Eustachian tube vs. Adult Eustachian tube |
|
The infant's Eust. tube is relatively shorter and wider and its position is more horizontal than that of the adults. So, it is easier for pathogens from the nasopharynx to migrate through to the middle ear. This lumen is surrounded by lymphoid tissue, which increases during childhood, this the lumen is easily occluded. These factors place the infant at greater risk for middle ear infections than adults. |
| |
|
Compare and contrast pathways of hearing: Air conduction vs. Bone conduction |
|
Bone conduction=the bones of the skull vibrate, and are transmitted directly to the inner ear and to the cranial nerve VIII.Air conduction=Sound waves produce vibrations that are carried by the middle ear ossicles to your oval window. Sound waves travel through the cochlea, which is coiled like a snail's shell, and are dissipated against the round window. Basilar membrane vibrates at a point specific to the frequency of the sound. Fibers along basilar membrane are the receptor hair cells of the organ of Corti. As hair cells bend, they mediate the vibrations into electric impulses, which are conducted to the auditory potion of cranial nerve VIII to brainstem
|
| |
|
Subjective vertigo |
|
occurs when the person feels like he or she is spinning |
| |
|
Objective vertigo |
|
occurs when the person feels like the room spins |
| |
|
Rinne Test |
|
Compares air conduction and bone conduction sound. Place the stem of the vibrating tuning fork on the person's mastoid process and ask him or her to signal when the sound goes away. Quickly invert the fork so the vibrating end is near the ear canal. The person should still hear a sound. Normally the sound is heard twice as long by air conduction (next to ear canal) as by bone conduction (through mastoid process). |
| |
|
Weber Test |
|
Valuable when a person reports hearing better with one ear than the other. Place a vibrating tuning fork in the midline of the person's skull and ask whether the tone sounds the same in both ears or better in one. The person should hear the tone by bone conduction through the skull, and it should sound equally loud in both ears. |
| |
|
Voice/Whisper Test |
|
Test one ear at a time while masking hearing in the other ear to prevent sound transmission around the head. Place one finger on the tragus and rapidly push it in and out of the auditory meatus. Shield your lips so the person cannot compensate for a hearing loss. With your head 30-60 cm from the person's ear, exhale and whisper slowly some two-syllable words. Normally, the person repeats each word correctly after you say it. |
| |
|
Subjective Data for Nose, Mouth and Throat |
|
Nose=any discharge, frequent colds, sinus pain, trauma, epitaxis (nosebleeds), allergies, altered smells?Mouth and throat=sores or lesions, sore throat, bleeding gums, toothache, hoarseness, dysphagia, altered taste, smoking/alcohol use, self-care behaviors |
| |
|
Inspect Nasal Cavity |
|
Note color of nasal mucosa and look for swelling, discharge, bleeding, and foreign objects. Observe the nasal septum for deviation, perforation, bleeding or foreign objects. Inspect turbinates for swelling or polyps. Sinuses are palpated for tenderness which could indicate chronic allergies, acute infection. Transillumination is used to look for inflamed sinus filled with fluid. If fluid present, you won't see the light. |
| |
|
Inspect Mouth |
|
Lips- Observe color, moisture, cracking, lesions. Abnormal findings=circumoral pallor, cyanosis, cherry red color, chelitis, and herpes. Teeth and gums=inspect the condition, note any bleeding indicating gingivitisTongue=note color, enlargement, whether saliva is decreased or excessive. Inspect for white patches or lesions. Buccal mucosa=check for color, nodules, or lesions. Palate=observe color which should be white in the anterior hard palate and pink in the posterior soft palate. Observe texture. Ask person to say ahh, to see the uvula and the soft palate rise in the midline, which tests one function of cranial nerve X, the vagus nerve. Throat=observe tonsils for redness and swelling, or large white spots which could be an acute infection. A white membrane covering tonsils may indicate mononuclesosis, leukemia, and diptheria. Also note size of tonsils. |
| |
|
Describe grading system used for swollen tonsils |
|
1+Visible2+Halfway between tonsillar pillars and uvula3+Touching the uvula4+Touching each other |
| |
|
Instruct client regarding risks of using smokeless tobacco |
|
SLT contains nicotine like cigarettes, and can lead to nicotine addiction and dependence. Main two types include chewing tobacco and snuff. The use of SLT has been associated with an even greater risk of cancers than smoking, including cancers of the pharynx, larynx, esophagus, and oral cancers. Other effects:tooth decayCADperipheral vascular dzhypertensionpeptic ulcer dzfetal morbiditygum recessionbad breathunhealthy eating habits
SLT is used more by white males. |
| |
|
Describe direction of blood flow from entering the heart and through the body |
|
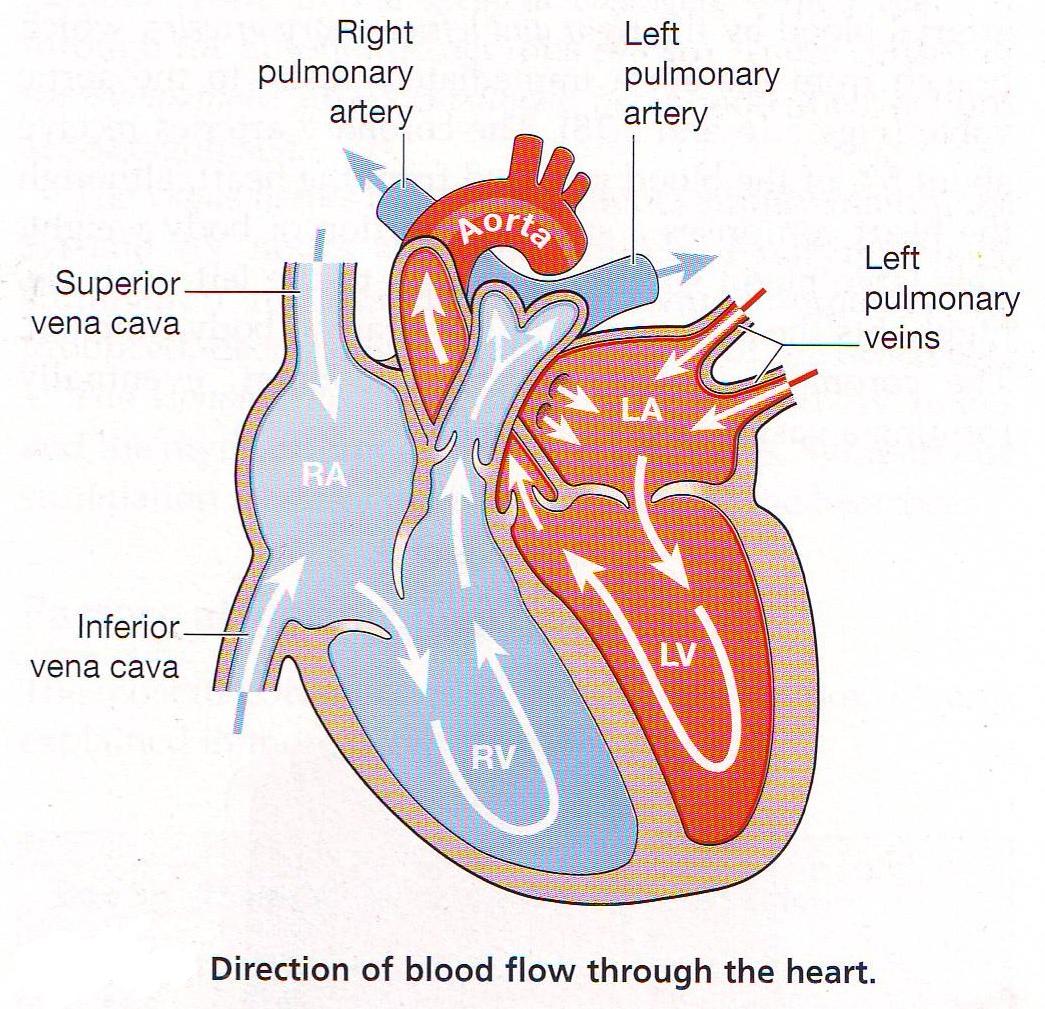
1. From liver to RA through inferior vena cava. Superior vena cava drains venous blood from head and upper extremities. From RA, venous blood travels through tricuspid valve to RV2. From RV, venous blood flows through pulmonic valve to pulmonary artery. Pulmonary artery delivers unoxygenated blood to lungs.3. Lungs oxygenate blood. Pulmonary veins return fresh blood to LA4. From LA, arterial blood travels through mitral valve to LV. LV ejects blood through aortic valve into aorta.5. Aorta delivers oxygenated blood to body.
|
| |
|
Identify normal heart sounds S1 and S2 |
|
S1=The closure of the AV valve and signals the beginning of systole.The AV valves close to prevent regurgitation of blood back up into atria during contraction.After ventricle contents are ejected, its pressure falls. When pressure falls below pressure in the aorta, some blood flows backward toward the ventricle, causing the aortic valve to swing shut. S2=This closure of the semilunar causes the second heart sound (S2) and signals the end of systole. |
| |
|
Compare and contrast characteristics of S1 and S2. |
|
S1 occurs with AV valve closure and signals beginning of systole (ejection phase). You can hear S1 over the precordium, but usually is loudest at apex. S2 occurs with closure of semilunar valves and signals end of systole. S2 is loudest at the base. S1 is louder than S2 at the apex, S2 is louder than S2 at the base. *S1 coincides with the carotid artery pulse and the R wave. |
| |
|
Identify characteristics of heart murmurs |
|
Caused by turbulent blood flood and collision currents. A murmur is a gentle, blowing swooshing sound that can be heard on the chest wall. Conditions resulting in a murmur are as follows:1. Velocity of blood increases (flow murmur), can be due to exercise, thyrotoxicosis2. Viscosity of blood decreases (like in anemia)3. Structural defects in valves (narrowed or incompetent valve) or unusual openings occur in the chambers |
| |
|
characteristics of a heart murmur (TLPQLRP) |
|
1. Timing=it is crucial to define murmur by its occurrence in systole or diastole. 2. Loudness= intensity in terms of 6 grades:i=barely audible, heard only in a quiet room with difficultyii=clearly audible, but faintiii=moderately loud, easy to heariv=loud, associated with a thrill palpable on chest wallv=very loud, heard with one corner of stethoscope lifted off the chest wallvi=loudest, still heard with entire stethoscope lifted off chest wallPattern=intensity may follow a pattern of crescendo-decrescendo, etcQuality=describes quality as musical, blowing, harsh or rumblingLocation=describe area of maximum intensity of murmur by noting valves or intercostal spaceRadiation=may be transmitted downstream in direction of blood flowPosture=some disappear or are enhanced with position changes. |
| |
|
Innocent vs. functional murmur |
|
Innocent=indicates having no valvular or other pathogenic cause. Usually soft, grade ii, midsystolic, short, crescendo-decrescendo and with vibratory or musical quality, disappears with sitting. Functional=due to increased blood flow in the heart*Treat all murmurs as if they were pathogenic until proven otherwise |
| |
|
Physiological effects of an aging heart |
|
Gradual rise in systolic blood pressure, while diastolic stays same, resulting in a widened pulse pressure. Some aging adults experience orthostatic hypotension (drop in BP when rising to sit or stand).
|
| |
|
Cultural aspects that affect cardiovascular system |
|
Heart dz and stroke are higher among black adults. Black and Mexican American women have higher cardio risk factors. |
| |
|
Major risk factors for heart dz and stroke= |
|
high blood pressuresmokinghigh cholesterolobesityphysical inactivitydiabetesoral contraceptives |
| |
|
Hypertension is more common andSerum cholesterol levels are higher than whites among ____ during childhood, but reverse in adulthood |
|
Blacks. |
| |
|
BMI of overweight person=BMI of obese person= |
|
25+30+ |
| |
|
Apical Pulse |
|
Location=should occupy only one interspace, either 4th or 5th, and be at the medial to midclavicular lineSize=1cm x 2cmAmplitude= short, gentle tapDuration= short, only first half of systole
*Listen to number of beats per minute |
| |
|
Carotid Pulse vs. Internal Jugular Pulse |
|
Internal Jugular
Pulse
Carotid Pulse
Location
Lower, more lateral, under or behind the
sternomastoid muscle
Higher and medial to this muscle
Quality
Undulant and diffuse, two visible waves per cycle
Brisk and localized, one wave per cycle
Respiration
Varies with respiration; its level descends during
inspiration when intrathoracic pressure is decreased
Does not vary
Palpable
No
Yes
Pressure
Light pressure at the base of the neck easily
obliterates
No change
Position of Person
Level of pulse drops and disappears as the person is
brought to a sitting position
Unaffected
|
| |
|
Apical Pulse vs. Apical Impulse |
|
Apical impulse=pulsation created as LV rotates against chest wall during systole. When visible, it occupies 4th or 5th intercostal spaces, at or inside midclavicular line. Normally it is 1cm x 2cm, a short, gentle tap and occupies first half of systole. Not palpable in obese personsApical pulse=sound of heart beating, count beats. |
| |
|
Name 5 areas of ausculatation of cardiac system |
|
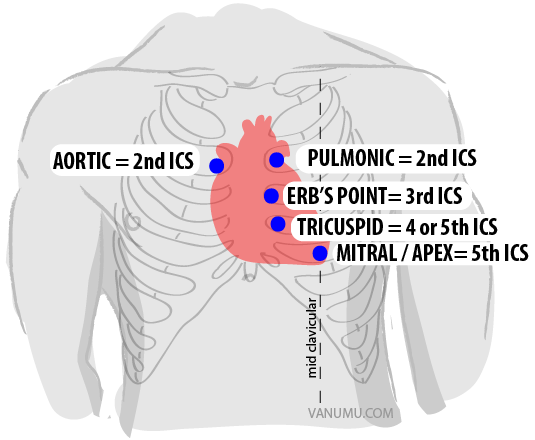
Aortic areaTricuspid areaPulmonic areaErb's pointMitral area |
| |
|
When should bell vs. diaphragm of stethoscope be used? |
|
Bell=used when auscultating carotid artery, and for relatively lower pitched sounds. Diaphragm=used for relatively higher pitched soundsUse both when auscultating traditional valve areas |
| |
|
Precordium |
|
=area on the anterior chest overlying the heart and major arteries and veins |
| |
|
When performing a regional cardiovascular assessment, use this order: |
|
1. Pulse and BP2. Extremities3. Neck vessels4. Precordium |
| |
|
Carotid Artery Exam |
|
Purpose=carotid artery yields important info about cardiac functionProcedure=1. palpate carotid artery (feel contour and amplitude of the pulse). Normally, contour is smooth with rapid upstroke and slower downstroke. ~2+. should be same bilaterally.2. auscultate carotid artery listening for signs of bruits (used for persons middle-aged+ or who show sx of cardio dz). Apply bell over carotid artery at:a. angle of jawb. midcervical linec. base of neckAsk person to take a breath and hold it briefly while you listen so that tracheal breath sounds don't mask or mimic carotid artery bruit.
|
| |
|
Jugular Vein Exam |
|
Purpose=used to assess central venous pressure and judge heart's efficiency as a pump. Procedure= 1. Inspect jugular venous pulse. Turn person's head slightly away from examined side and direct light tangently onto neck to highlight pulsations and shadows. Look for pulsations of internal jugular veins in area of suprasternal notch or around origin of sternomastoid muscle around clavicle. 2. estimate jugular venous pressure. |
| |
|
Precordium Exam |
|
Purpose=to evaluate apical impulse and valve sounds and function. Procedure=1. Inspect anterior chest for pulsations (4th or 5th intercostal space)2. Palpate apical impulse (point of maximal impulse). Ask person to exhale and hold it. Note location, size, amplitude, and duration. Apical impulse is decreased in obese persons, and increased with high cardiac output states (anxiety, fever, hyperthyroidism, anemia). 3. Palpate across precordium searching for any other pulsations (normally none exist). 4. Auscultation=Start at apex and listen at 5 valve areas in Z pattern, being with diaphragm and repeat with bell. Listen for murmurs or abnormal heart sounds, listen to S1 and S2. Listen in supine and then laying on side. |
| |
|
Raynaud's Phenomenon |
|

progressive tricolor (pallor, cyanosis, rubor) change of the fingers in response to cold, vibrations or stress |
| |
|
Lymphedema |
|

removal of lymph nodes with breast surgery, or damage to lymph nodes and channels can impede drainage of lymph, causing build up of fluid in interstitial spaces.
|
| |
|
Arteriosclerosis-Ischemic ulcer |
|
buildup of fatty plaques on intima plus hardening and calcification of arterial wall |
| |
|
Venous Stasis Ulcer |
|
occurs after DVT or chronic incompetent valves in deep veins |
| |
|
Superficial Varicose Veins |
|
incompetent valves permit reflux of blood, producing dilated, tortuous veins. Hydrostatic pressure causes distal valves to be incompetent and causes worsening of varicosity. |
| |
|
DVT |
|
Deep Vein Thrombosis. deep vein occluded by a thrombus, causing inflammation, blocked venous return, cyanosis, and edema. |
| |
|
atherosclerosis |
|
chronic build up of fatty streaks, fibroid plaque, calcification of vessel wall and thrombus formation.
|
| |
|
Aneurisms |
|
a sac formed by dilation in artery that weakens the middle layer of the vessel wall. This stretches the inner and outer layers and the effect of BP creates the balloon enlargement. |
| |
|
Pulse Ratings |
|
3+ Bounding2+ Normal1+ Weak0 Absent |
| |
|
Arteries |
|
Pump oxygenated blood to body; A high pressure system. Contain elastic and smooth muscle fibers, which control the amount of blood that's delivered to the tissues. |
| |
|
Ischemia |
|
deficient supply of oxygenated arterial blood to a tissue caused by obstruction of a blood vessel |
| |
|
Pulse points accessible during examinations |
|
Temporal=palpate in front of earCarotid=groove between sternomastoid muscle and tracheaBrachial=supplies the arm, runs in the biceps-triceps furrow of upper arm and surfaces at the antecubital fossa in elbow medial to biceps tendonRadial=medial to radius at wristUlnar=medial to ulna, but deeper and difficult to feelFemoral=passes under inguinal ligament down thighPopliteal=part of femoral artery travels down lower thigh and runs posteriorly behind kneeDorsalis pedis=on dorsum of foot
|
| |
|
Veins |
|
more veins that arteries, lie closer to surfacelarger in diameter, thin walls, more expandabledrain deoxygenated blood and its waste products and return it to the heartlow pressure system bc no pump to generate blood flow
|
| |
|
Capacitance vessels |
|
refers to vein's ability to compensate for stress on heart by stretching to hold more blood volume |
| |
|
Mechanisms of venous blood flow |
|
1. Contracting skeletal muscles that milk blood proximally back toward heart (i.e. calf pump when walking)2. pressure gradient caused by breathing3. intraluminal valves which ensure unidirectional flow toward heart |
| |
|
Assessing edema |
|
1. Note location and level of edema2. Levels of pitting: a. 1+ mild pitting, slight indentation, no perceptible swellingb. 2+ moderate pitting, indentation subsides rapidlyc. 3+ deep pitting, indentation remains for a short time, leg swollend. 4+ very deep pitting, indentation lasts a long time, leg very swollen |
| |
|
Maneuvers that may help to locate difficult pulses more easily |
|
1. Femoral=ask person to bend their knees to the side like a froglike position. Press firmly and then slowly release, noting pulse tap under your fingertips2. Popliteal=With leg extended but relaxed, anchor your thumbs on knee and curl fingers around into popliteal fossa. Press fingers forward hard to compress artery against bone. Can turn person face down and lift up lower leg. Posterior tibial= curve fingers around medial malleolus. you will feel tapping right behind it in grove btwn alleolus and achilles tendon.Dorsalis pedis=requires very light touch. Is usually just lateral to extensor tendon of big toe. |
| |
|
6 symptom for arterial insufficiency (6Ps) |
|
PainPallorPulselessnessParesthesia (tingling sensation, numbness, prickling)Poikilothermia (coldness)Paralysis
|
| |
|
Abnormal variations of pulses1. Thready/weak=2. Full, bounding=3. Water-hammer (Corrigan's pulse)=4. Pulses Bigeminus=5. Pulsus Alterans=6. Pulsus Paradocus= |
|
1. 1+ hard to palpate, need to search for it2. 3+ easily palpable, pounds
|
| |
|
3. Water-hammer (Corrigan's pulse)= |
|
= 3+, greater than normal force, then collapses suddenly |
| |
|
4. Pulses Bigeminus= |
|
4. Pulses Bigeminus= rhythm is coupled, every other beat comes early, or normal beat followed by a premature beat. Force of premature beat is decreased bc of shortened cardiac filling times. |
| |
|
5. Pulsus Alterans= |
|
5. Pulsus Alterans=rhythm is regular, but force varies with alternating beats of large and small amplitude |
| |
|
6. Pulsus Paradocus= |
|
6. Pulsus Paradocus=beats have weaker amplitude with inspiration, stronger with expiration |
| |
|
7. Pulsus Bisferiens= |
|
7. Pulsus Bisferiens=each pulse has two strong systolic peaks, with a dip in between. |
| |
|
Manual compression test |
|
tests the competence of the valves in the varicose vein. while the person is standing, place one hand on the lower part of the varicose vein, and compress the vein with your other hand about 15-20 cm higher. competent valves will prevent a wave transmission and your lower fingers will feel no change. |
| |
|
Color change |
|
sluggish return to color suggests occlusion of collateral arterial flow |
| |
|
Homan's sign |
|
flex person's knee, then gently compress calf muscle against tibia. no tenderness should be present. Dorsiflex foot toward tibiaPain=positive=probably DVT
|
| |
|
Modified Allen's Test |
|
used to evaluate adequacy of collateral circulation prior to cannulating radial artery. three steps:a. depress radial and ulnar arteries by opening and closing fistb. Normal blood returns via ulnar arteryc. occluded ulnar artery shows no blood return |
| |
|
Note specific lymph nodesCervicalAxillaryEpitrochlearInguinal |
|
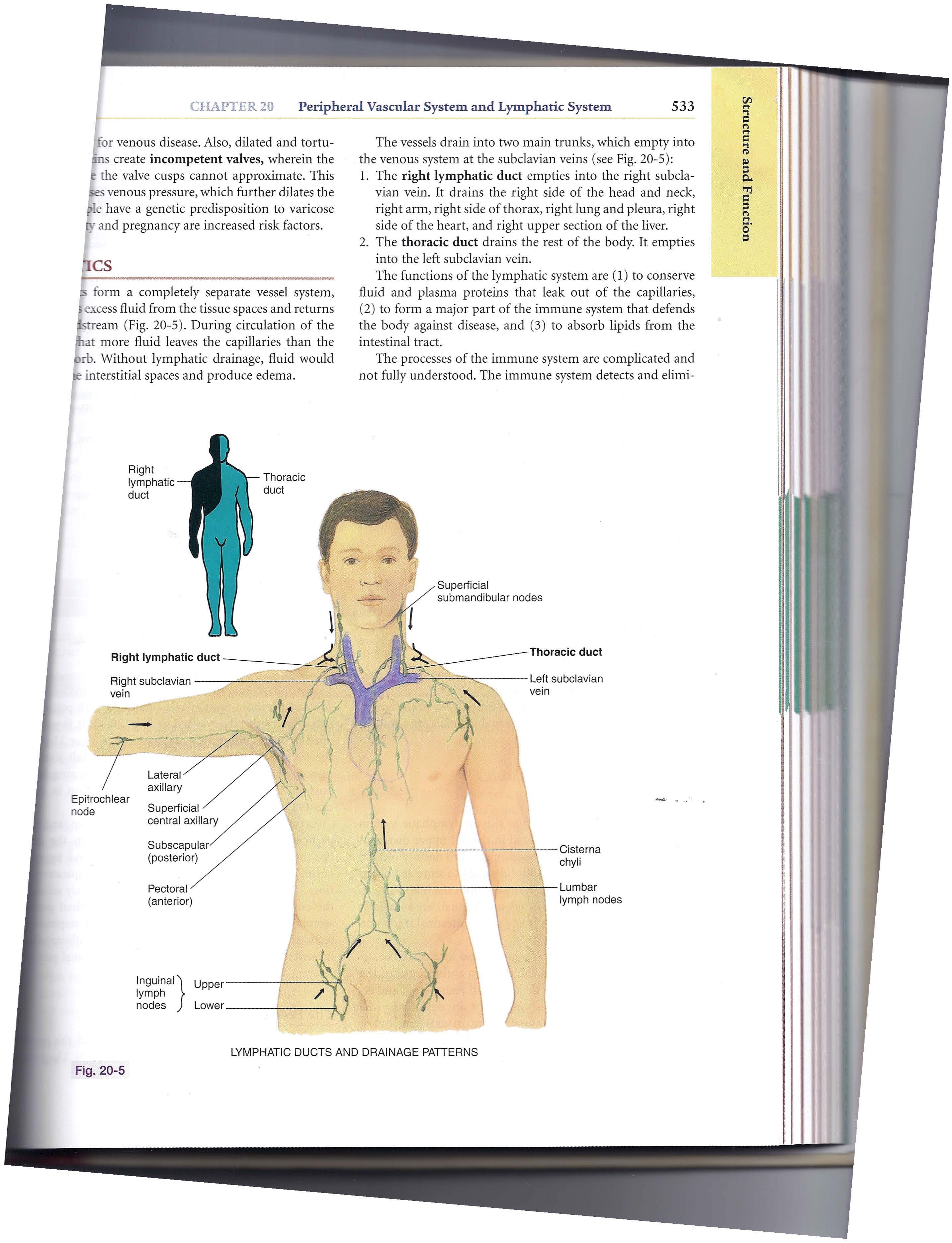
See image |
| |
|
Cervical lymph nodes |
|
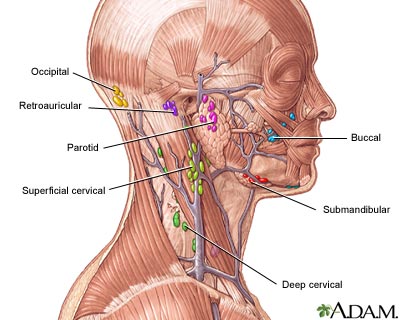
see image |
| |
