|
What are the two halves of circulation and what are their main function? |
|
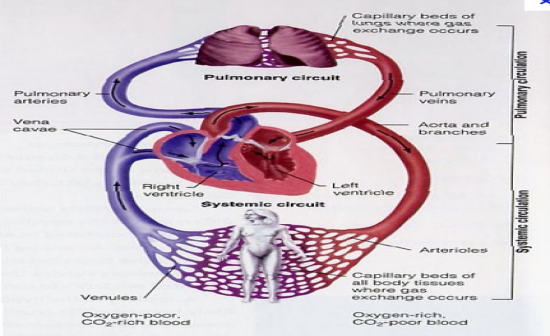
Systemic Circulation: (Left ventrical --> Right Atrium) Carries oxygenated blood away from the heart to the body, and returns deoxygenated blood back to the heart.
Pulmonary Circulation: (Right Ventrical --> Left Atrium). Carriesoxygen-depleted blood away from the heart, to the lungs, and returns oxygenated (oxygen-rich) blood back to the heart.
|
| |
|
What part of the circulatory system can create great resistance to flow? When would this action be needed? |
|
Arterioles: Has great variation in diameter due to their muscular walls, and are the primary site of vascular resistance.
Exercise: To increase bood flow to skeletal muscle via vasodilation (decreasing resistance). |
| |
|
What facrots regulation resistance? |
|
Flow = Pressure Gradient + Resistance to flow (Ohms Law)
MAP = Change in pressire
MAP = CO x TPR
- Hence if the MAP is maintained failry constant, the blood flow to any muscular bed is deendent only on the vascular resistance (mainly arterial resistance) |
| |
|
What is Tidal Volume (VT)? |
|
The amount of air entering (or leaving) the mouth and nose in one breath. = ~.5L |
| |
|
What is the VO2? |
|
The Amount of O2 absorbed into the pulmonary blood/min. |
| |
|
Why is the partial pressure of O2 in arterial blood closely match the partial pressure of O2 in the Alveoli? |
|
Because of extremely rapid exchange of O2. |
| |
|
How does O2 and CO2 move? |
|
Diffusion down pressure/concentration gradient |
| |
|
How do the tissues get the right supply of O2? |
|
Feedback system matches supply to demand bia two mechanisms:
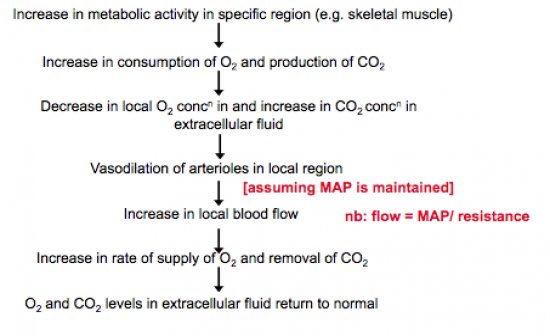
(1) Metabolic regulation of local vascular resistance
(2) Maintenance of perfusion pressure (MAP) by feedback control system. |
| |
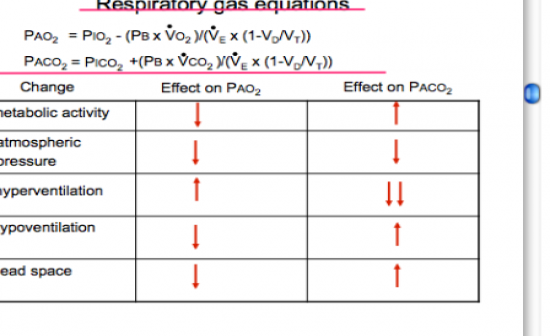
How do changes to:
a) Increased metabolic activity
b) Decreased atmospheric pressure
c) Hyperventilation
d) Hypoventilation
e) Increased dead space
Effect PO2 and PCO2? |
|
|
| |
|
Draw a flow diagram outlining the main response to increased metabolic activity. (6 steps) |
|
|
| |
|
Describe the Baroreflex Pathway? |
|
Inputs from receptors which signal changes in blood pressure go to the brain and reflexly influence the activity of sympathetic nerves to the heart and blood vessles. |
| |
|
Describe the Baroreflex? |
|
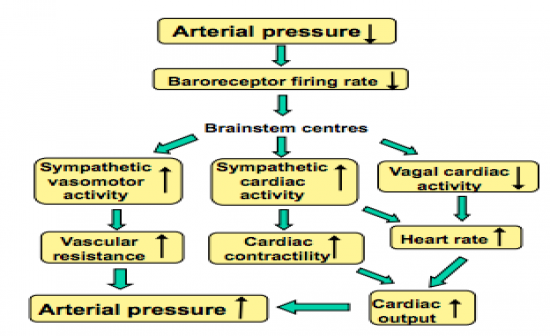
The baroreflex or baroreceptor reflex is one of the body's homeostatic mechanisms for maintaining blood pressure (STRETCH SENSITIVE). It provides a negative feedback loop in which an elevated blood pressure reflexively causes heart rate to decrease therefore causing blood pressure to decrease; likewise, decreased blood pressure activates the baroreflex, causing heart rate to increase thus causing an increase in blood pressure. |
| |
|
Which fibre type (myelinated or unmyelinated) have a higher threshold and saturation point? |
|
A. Unmyelinated:
Unmyelinated fbres show little adaption when pressure levels are high, and hence making unmyelinated fibres better able to signal sustained long term changes in arterial presure. |
| |
|
What does resetting the baroreflex mean? |
|
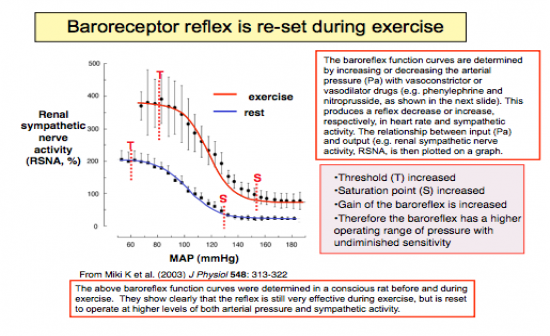
The baroreflex can be reset during exercise/sleep, to regulate the arterial pressure around whatever the apropriate pressure requires.
Eg during exercise, the curves are shifted to a higher operating range, eg your BP is increased but the baroreceptor re-adjusts/reset around a higher MAP. |
| |
|
What are the two types of atrial receptors and when do they fire? |
|
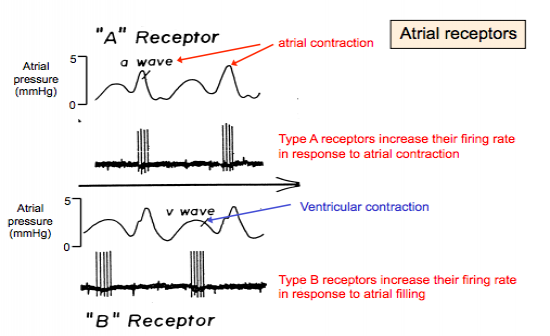
Type A: Increase their firing rate in response to atrial contraction.
Type B: Increase their firing rate in response to atrial filling |
| |
|
What is a Haemorrhage, and what is the bodies compensatory response? |
|
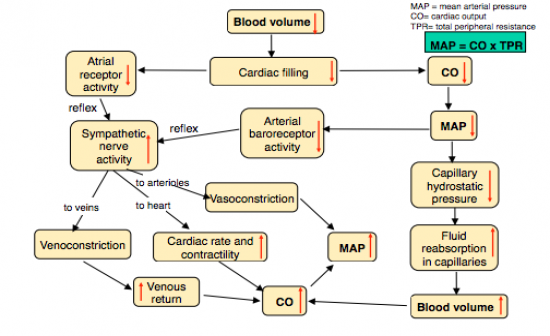
Haemorrhage: Loss of a large amount of blood, which lowers the blood volume.
Compensatory response: See image |
| |
|
What triggers the release of Vasopressin? And what effect does it have? |
|
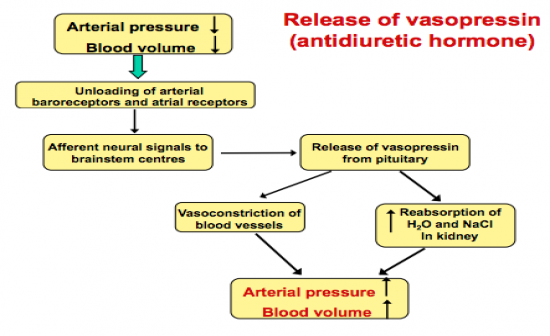
Triggered: Drop in blood pressure or Drop in blood volume.
Response: Acts to increase blood pressure and blood volume to normal levels - See image |
| |
|
What receptor fires in response to changes in the partial pressure of oxygen, and where are they located? |
|
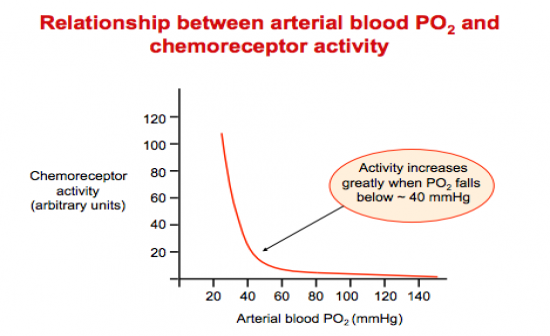
A. Chemoreceptors, in the carotid body.
Activity increases greatly when PO2 falls below ~40mmHg - See image |
| |
|
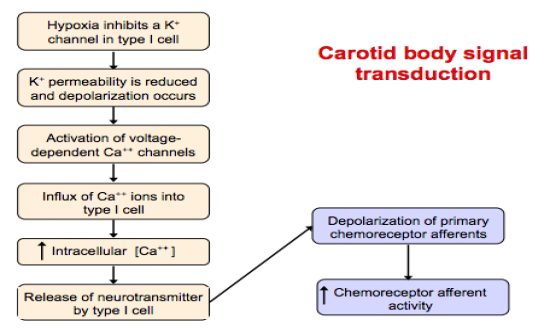
Describe the Transduction Method in the Carotid Body? (8 steps) |
|
|
| |
|
What is hypoxia? And what is the chemoreceptors reflex response to this? |
|
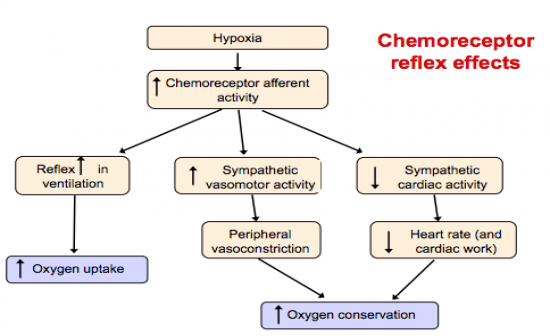
Hyppoxia: The partial pressure of O2 falls below normal (~90-100mmHg) causing excitation of the chemoreceptors.
Chemoreflex: See Image |
| |
|
What are the Ergoreceptors and where are they located? |
|
Ergoreceptors are the receptors located in the skeletal muscles. They can be either mechanoreceptors or chemoreceptors, and are activated during exercise. |
| |
|
What is the exercise pressor reflex and how do the ergoreceptors influence this? |
|
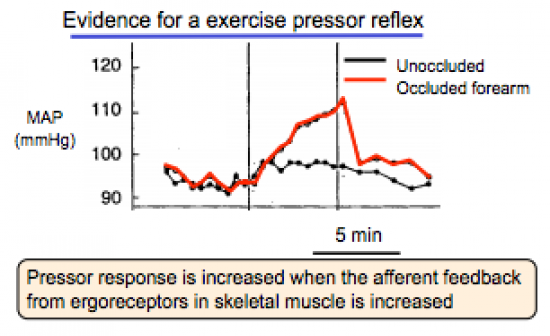
Exercise Pressor Reflex: The exercise pressor reflex is believed to play a role in causing the cardiovascular and ventilatory responses to exercise.
The pressor response is increased when the afferent feedback from the ergoreceptors in skeletal muscles is increased. |
| |
|
Describe the Diving Reflex (Nasopharyngeal reflex)? |
|
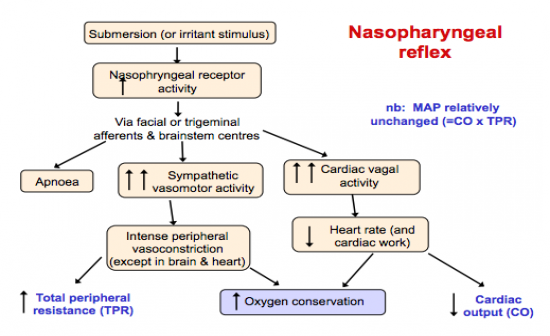
Diving reflex: Increase Depth = Decrease in HR
|
| |
|
How does the nasopharyngeal reflex interact with the chemorereceptors and pulmonary stretch receptors? And what is their combined outcome? |
|
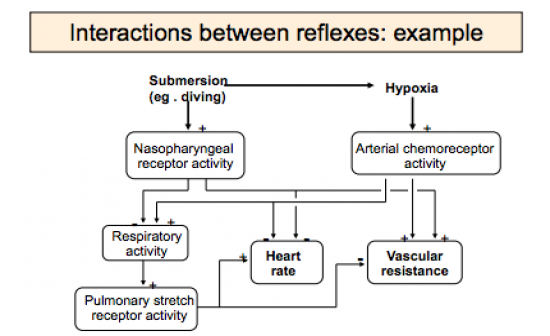
Chemoreceptor stimulation normally increases respiratory activity, but in presence of inputs from nasopharyngeal receptors apnoea occurs. But chemoreceptor and nasopharyngeal inputs summate to further increase reflex effects on vascular resistance and heart rate.
When respiratory activity increases, inputs from pulmonary stretch receptors tend to reflexly decrease heart rate and vascular resistance. |
| |
|
What is the bodies sympathetic response to dynamic exercise? (BP, TV, HR, MAP) |
|
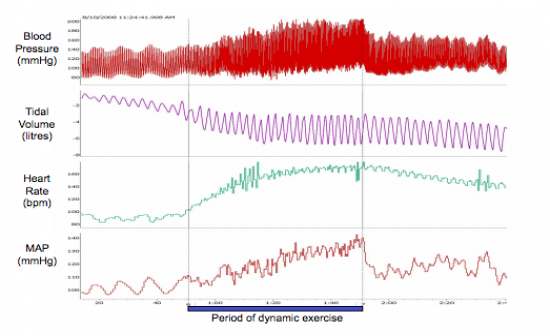
Bood Pressure: Increase
Tidal Volume: Increase
Heart Rate: Increase
Mean Arterial Pressure: Increase |
| |
|
Describe the relationship between Cardiac Output and Oxygen consumption. |
|
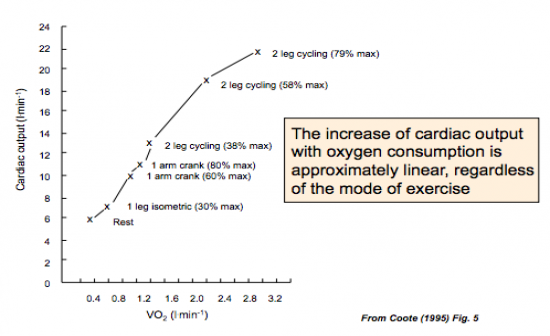
LINEAR: The increase of cardiac outut with oxygen is approximately linear, regardless of the mode of exercise. (If they increase simultaneously they must be due to similar mechanisms) |
| |
|
How is cardiac output redistributed during exercise? |
|
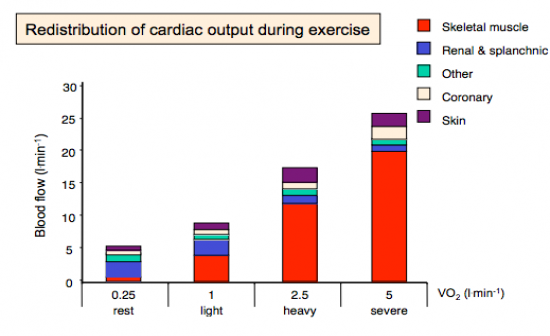
Large increase CO to skeletal muscle and heart
Decrease CO to renal
Increase to skin, but only at moderate exercise (thermoregulation), at severe exercise there is more demand for skeletal muscle. |
| |
|
What is the difference between isometric exercise and dynamic exercise? |
|
Isometric: Without moving limbs (eg holding weights)
Dynamic exercise: moving limbs (eg cycling) |
| |
|
Describe the 2 phases of changes to blood flow at the onset of exercise. |
|
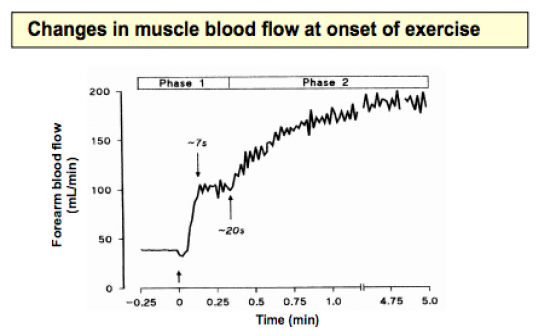
Phase I: Rapid increase initially (caused by muscle pump)
Phase II: Gradual increase |
| |
|
What is endotherlium derived relaxation factor (EDRF) and what experiment lead to this discovery? |
|
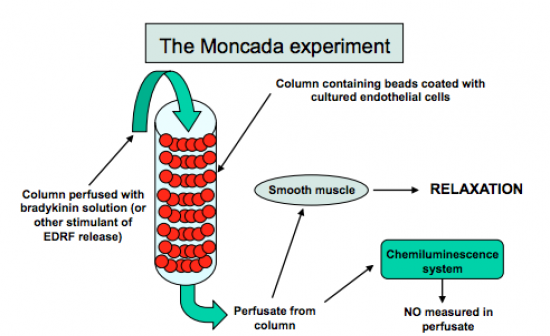
EDRF = Nitric Oxide
Nitric Oxide (found in amyl nitrate): Has a vasodilatory effect - Decreases BP.
The Monchada Experiment (1988): showed that endothelial cells make NO from arginine, which is converted to L-citrulline and then quickly recycled back to arginine.
Hence showed EDRF = NO |
| |
|
Draw a diagram describing the cellular mechanisms of NO formation and action. |
|
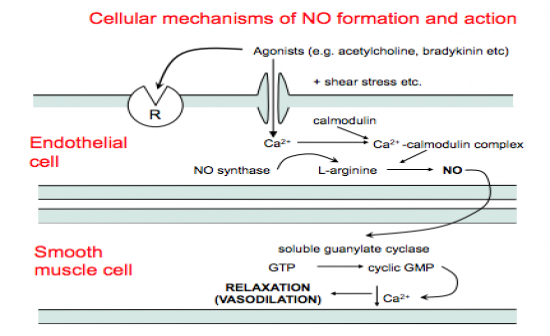
See image |
| |
|
What triggers the release of NO? |
|
- Not in blood: ACh, serotonin, substance P
- Arterial stretch causes the release of NO
- Increase in arterial blood flow triggers release of NO
|
| |
|
Define Hyperaemia and some of its causing mechanisms. |
|
Hyperaemia: The increase of blood flow to different tissues in the body.
1. Mechanical Mechanism: Muscle Pump
- Contraction of skeletal muscles compress veins which together with venous valves cause blood flow towards the heart - Happens immediately at onset of exercise and hence accounts for the initial rapid increase in blood flow at onset of exercise
2. Substance release from skeletal muscles:
- 5-10 seconds after onset of exercise, vasodilator substances are released from skeletal muscles (eg NO)
3. Substances transpported by blood:
- NO bind to oxyhaemoglobin and are released when O2 is released in exercising muscles.
4. Substances released from nerves:
- Ah spillover from motor nerves may cause vasodilation
ALL TOGETHER:
- Skeletal muscle pump causes initial rise in flow immediately after onset of exercise
- K+ ions from skeletal muscles may then contribute
- Substances released by skeletal muscles in proportion to contractile activity then play a role
- Flow induced release of vasodilators from endothelium may also contribute |
| |
|
What is the main function of the Rostral Vento Lateral Medulla (RVLM)? |
|
The RVLM are the key group of neurons for maintaining resting sympathetic activity. They recieve inputs from a wide variety of peripheral receptors, and peoject directly to the spnal sympathetic outflow. Hence the RVLM is a critical component of baroreceptor and other cardiovascular reflex'. |
| |
|
The blood CO2 level is the major factor that drives breathing. Where is the CO2 level sensed and how does it drive breathing? |
|
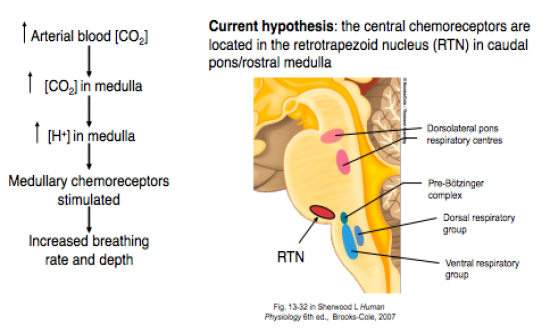
Curent hypothesis: Medullary chemoreceptors drive breathing - the central chemoreceptors are located in the retotrapezoid neucleus (RTN) in caudal pons/rostral medulla.
See Image. |
| |
|
Arterial hypoxia (a fall in blood O2 level) can also stimulate breathing. Where is the blood O2 level sensed and how does it drive breathing? |
|
FInd answer: |
| |
|
Breathing increases during exercise, fear or arousal. What mechanism causes that? (not blood O2 or CO2 levels) |
|
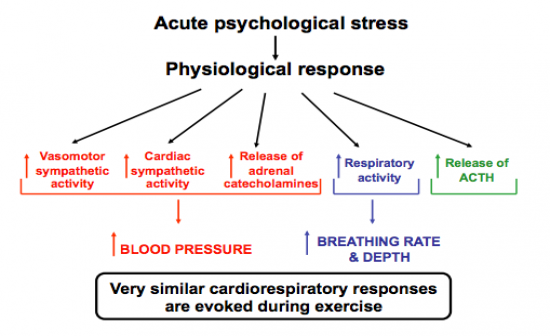
Different emoitions in humans are associated with different patterns of somatomotor and autonomic changes.
Acute psychological stress can result in physiological response - See image
Eg study looking at the cardiovascular response to emotional stress in a novice parachute jumper showed respiratory rate to increase simultaneously with increased heart rate, sugesting they are caused by the same neural mechanism/pathway. --> This is the DMH (Dorsomedial Hypothalamus)
The DMH is the key neuclei in regulating the cardiovascular response to stress. |
| |
|
What generates the basic respiratory rhythm? |
|
The basic respiratory rhythm is generated by neurons (nerve cells) within the lower brain stem. The group of cells is collectively called the respiratory centre.
Inspiration initiated by Increased firing rate |
| |
|
Descrive the pacemaker theory. |
|
Neurons in the medulla generate their own regular rhythm. |
| |
|
Descrive the central pathways subserving sympathetic and hormonal response to haemorrhage. |
|
See Image |
| |
